Why Aren’t Angioplasty Heart Stents More Effective?
Most heart attacks are caused by nonobstructive plaques that infiltrate the entire coronary artery tree. There is no such thing as “1-vessel disease,” “2-vessel disease,” […]
 ValVades
ValVades

Most heart attacks are caused by nonobstructive plaques that infiltrate the entire coronary artery tree. There is no such thing as “1-vessel disease,” “2-vessel disease,” or “left main disease.” Atherosclerotic plaque is continuous throughout the coronary arteries of heart attack victims.
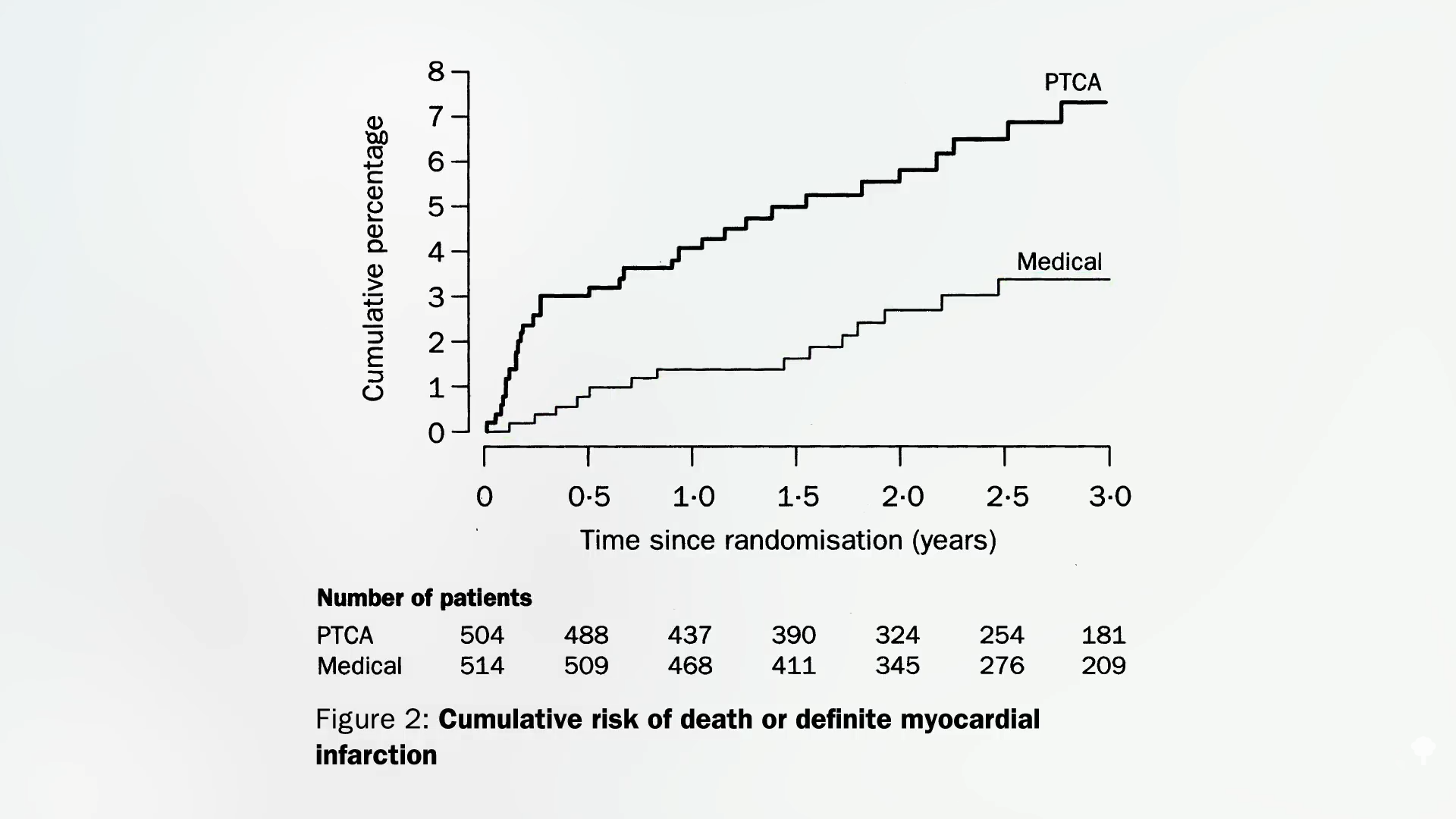
In angioplasty, a tiny balloon is inserted into a narrowed coronary artery that feeds the heart to force it to open wider to improve blood flow. It wasn’t put to the test in a randomized controlled trial until 1992. It not only failed to prevent heart attacks, but it also failed to show any survival benefit. However, the researchers only followed patients for six months and included people with relatively minor diseases who might not have been sick enough to benefit from the procedure. Enter the MASS trial. Researchers enrolled those with severe blockage high up in their left anterior descending coronary artery—the widow-maker or widower-maker (since coronary artery disease is also the number one killer of women)—and followed them for years. The findings? There was no difference in subsequent mortality or heart attack rates. There were only about 200 patients in that trial, though. Maybe the benefit was so subtle that a greater number of patients were needed to tease out the effect. Enter the RITA-2 study, which randomized more than a thousand patients. Researchers did indeed find a clear difference in the risk of future death and heart attack, but it was in the wrong direction. The angioplasty group suffered twice the risk compared to those randomized to forgo surgery, as shown below and at 1:18 in my video Why Angioplasty Heart Stents Don’t Work Better.
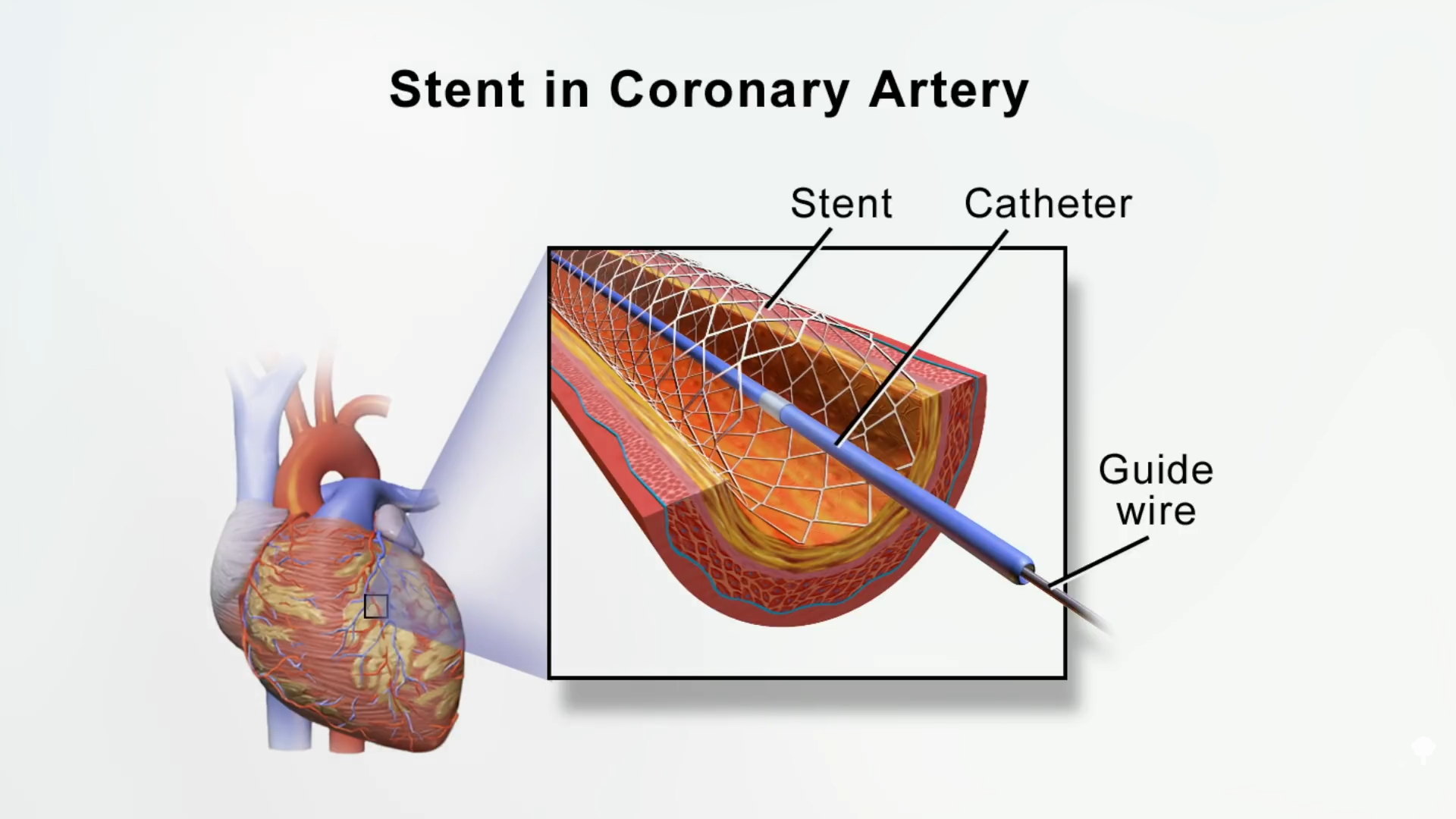
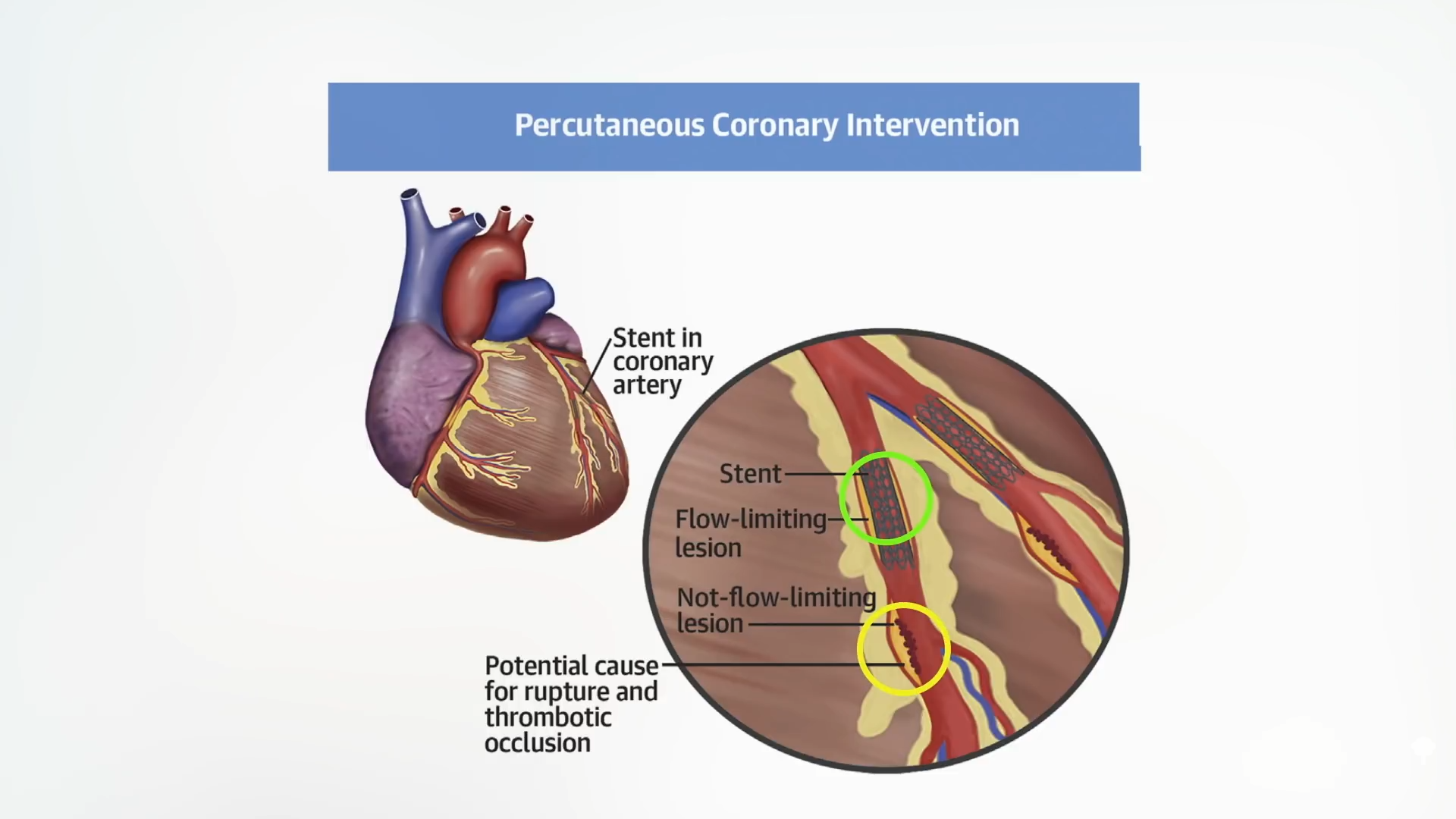
This was all before stents came into vogue, though. Instead of just ballooning up the artery, how about permanently inserting a stent, a metal mesh tube, to prop open the artery, as you can see here and at 1:33 in my video? Surely, that’s got to help.
Enter the MASS-II trial, which, again, saw no benefit after one year—but no benefit was seen after five years or even ten years. Then came the Courage Trial, which randomized thousands of patients, and it, too, fell flat on its face.
Those mostly used bare metal stents, though, not the newer “drug-eluting” ones that release drugs slowly. And what about high-risk groups, such as those diagnosed with diabetes and other more serious diseases, or those who have 100 percent blocked arteries days after having a heart attack? In meta-analysis after meta-analysis, looking at five trials with 5,000 patients, there was no reduction in death, heart attack, or even angina pain. In ten trials with more than 6,000 patients, there was no benefit for survival, heart attacks, or pain relief. Now, we’re up to more than a dozen major trials and nothing: no benefit from angioplasty and stents. “Furthermore, multiple analyses have failed to identify a single high-risk subset that benefits…” How is that possible? You’re physically opening up blood flow.
The reason it doesn’t work is that the majority of heart attacks in real life are caused by narrowings less than 70 percent—“i.e., most likely non-flow-limiting lesions”—so the plaques in our arteries that kill us tend not to be the ones that are restricting blood flow. Shown below and at 3:21 in my video are two atherosclerotic plaques. The one circled in green and labeled “Flow-limiting lesion” is squeezing off the blood flow so much that it can be seen on an angiogram and doctors can go after it with a stent.
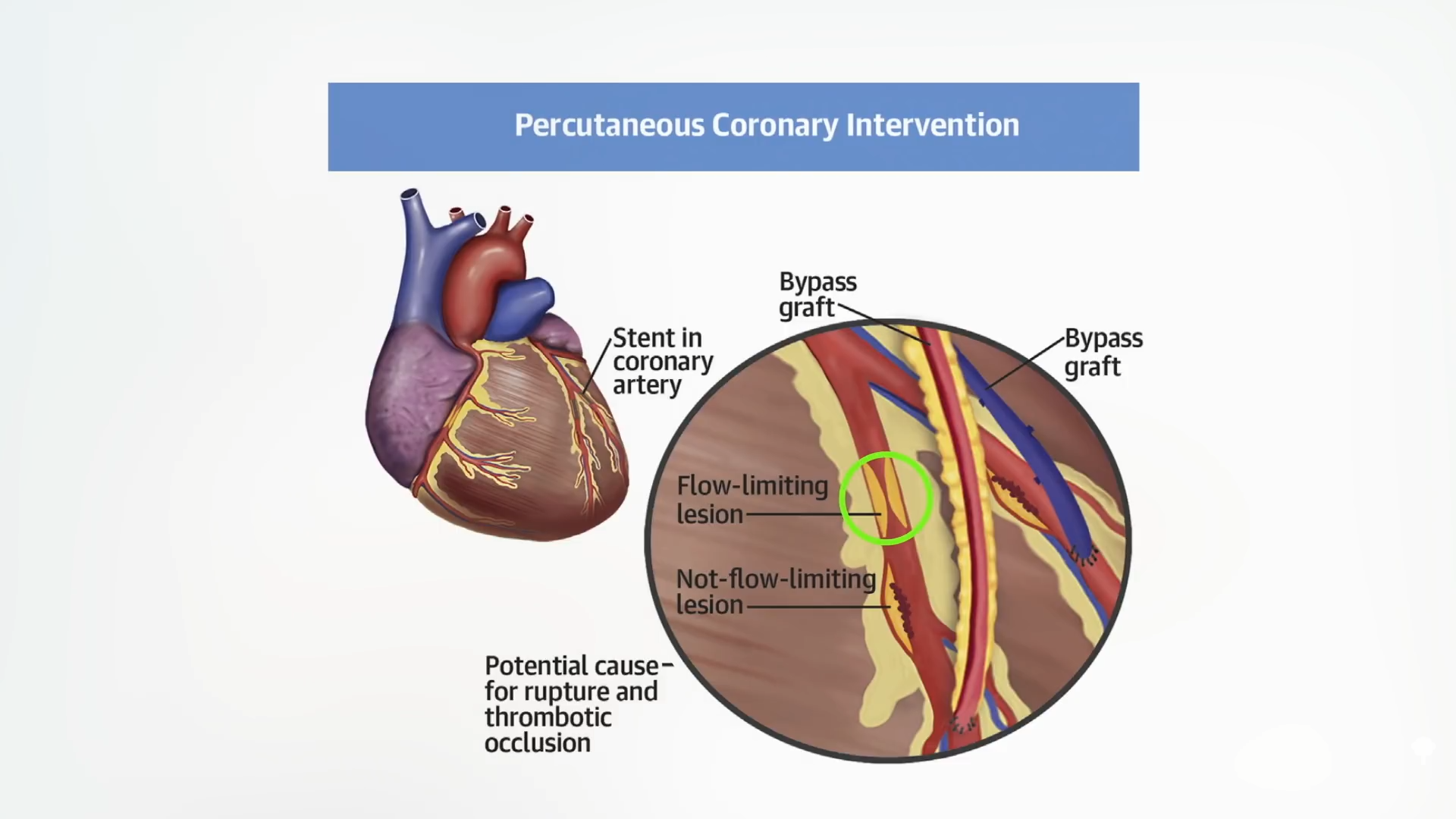
Problem solved and life saved, right? No, because it was the invisible one (circled in yellow below) that wasn’t even impeding blood flow that was going to kill us all along, as you can see here and at 3:27.
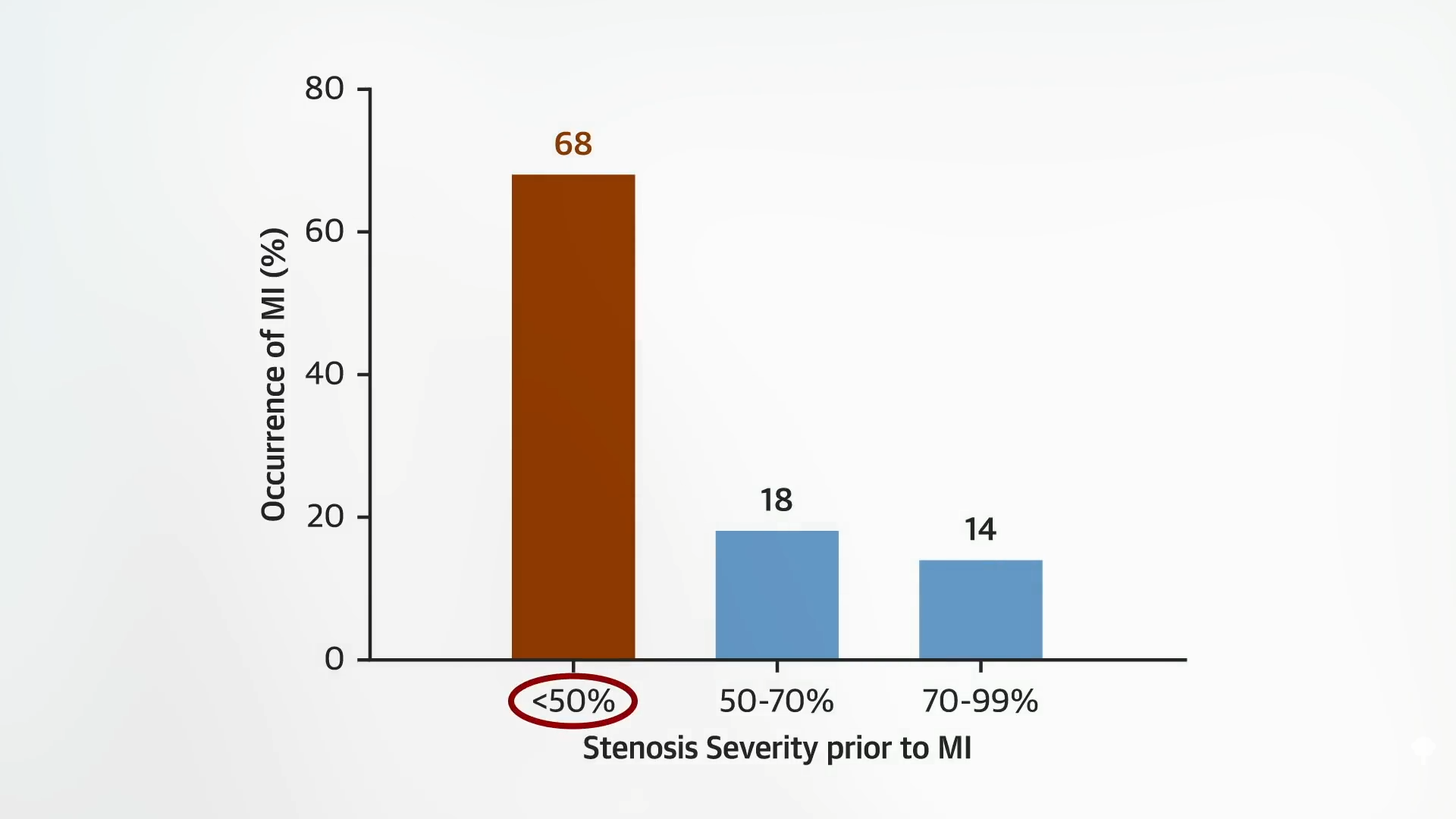
Indeed, most heart attacks are caused by nonobstructive plaques that don’t even cut blood flow by 50 percent, as seen below and at 3:40 in my video.
There’s a misconception, a “clogged pipe analogy of stable coronary heart disease [that] has been particularly difficult to dislodge,” in which cholesterol plaques slowly and inexorably encroach on blood flow, eventually cutting it off completely and triggering a heart attack. In reality, “coronary artery disease…is an inflammatory disease in which cholesterol from the blood is deposited in artery walls, causing an inflammatory reaction, like a pimple. When those pimples pop, they cause the blood in the arteries to clot at the site…Before rupture, these plaques often do not limit flow and may be invisible to angiography and stress tests. They are, therefore, not amenable to percutaneous coronary intervention (PCI),” that is, to angioplasty and stents. Old plaques are like “scarred old pimples.”
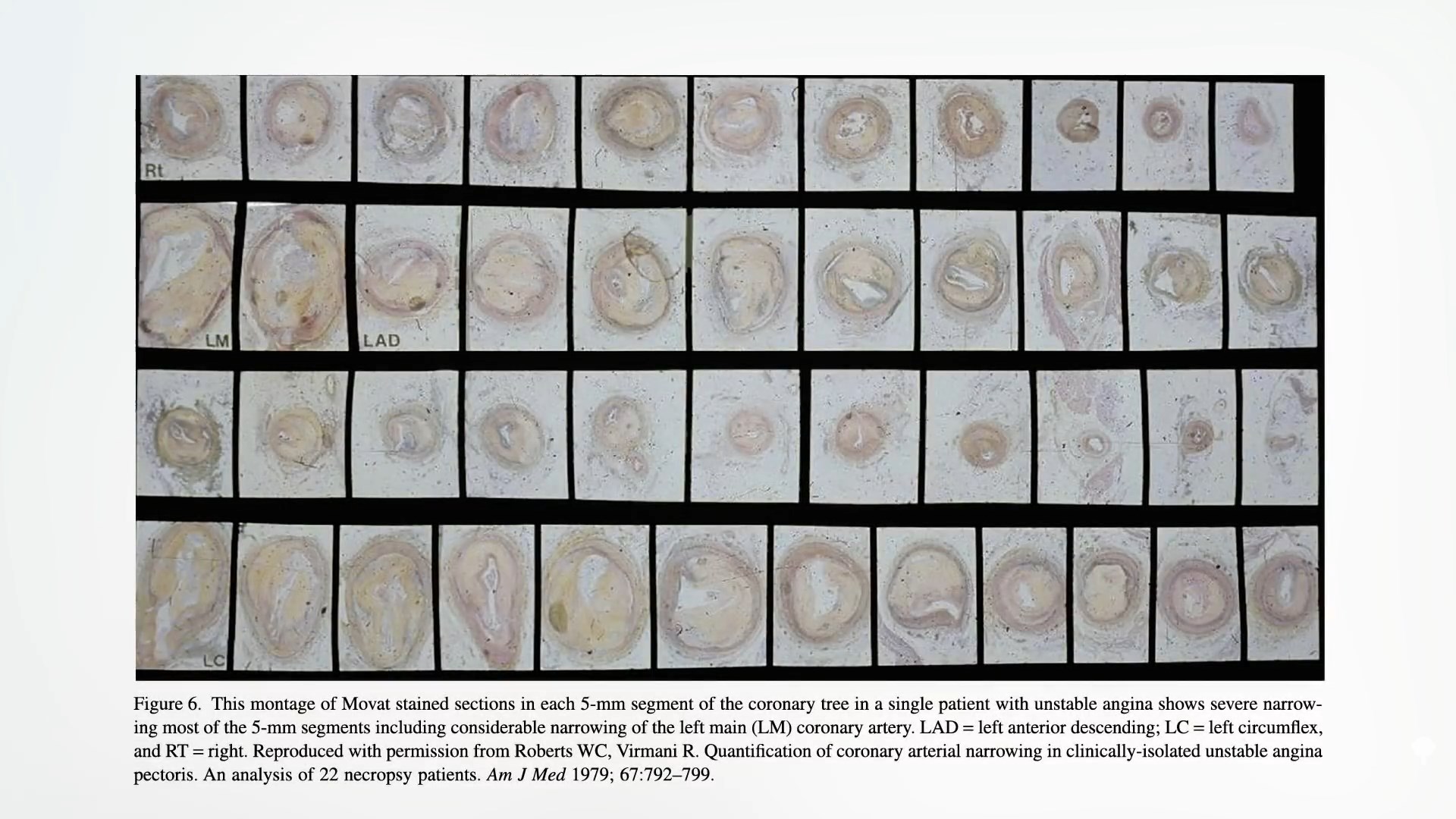
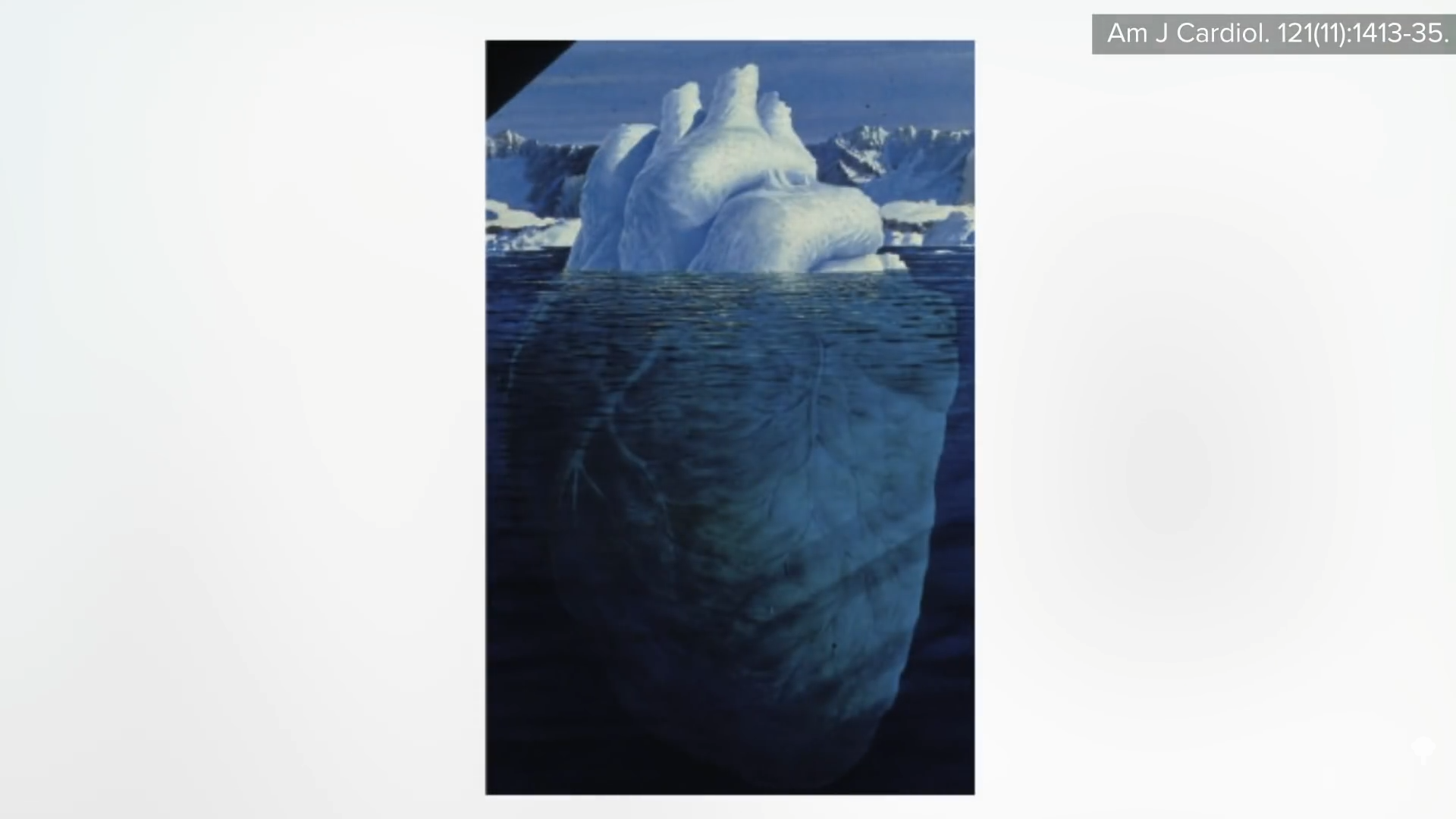
The tightest blockages are made up of mostly calcified and dense fibrous scar tissue. They can still rupture and kill us, but there are so many more of the smaller lesions brewing, which are hidden from view. The way we visualize coronary arteries is with an angiogram. X-rays are taken after a black-looking dye is injected into the arteries, so we can only see plaques that encroach on the blood flow. That’s why we get these kinds of tip-of-the-iceberg illustrations, the point of which “is to emphasize that most of the atherosclerotic plaque in the coronary arteries is not seen well by angiography,” as you can see below and at 4:49 in my video. To really understand what’s going on in people’s arteries, we must turn to autopsy. William Clifford Roberts is probably the most pre-eminent cardiovascular pathologist in the world. What did he learn after studying coronary arteries for 50 years? After examining nearly 2,000 bodies, he learned that atherosclerosis is a systemic disease.
“In patients with fatal coronary artery disease…the quantity of plaque is enormous. There is not just 1 plaque here, another plaque there, with normal lumen [clean arteries] between plaques. Plaques are continuous! Not a single 5-mm segment is devoid of plaque” in the entire coronary artery tree. So, says Dr. Roberts: “Isolated coronary disease is a myth. There are no such things as ‘1-vessel disease,’ and ‘2-vessel disease.’ Plaque is in all of the epicardial coronary arteries if it is in 1 of them.”
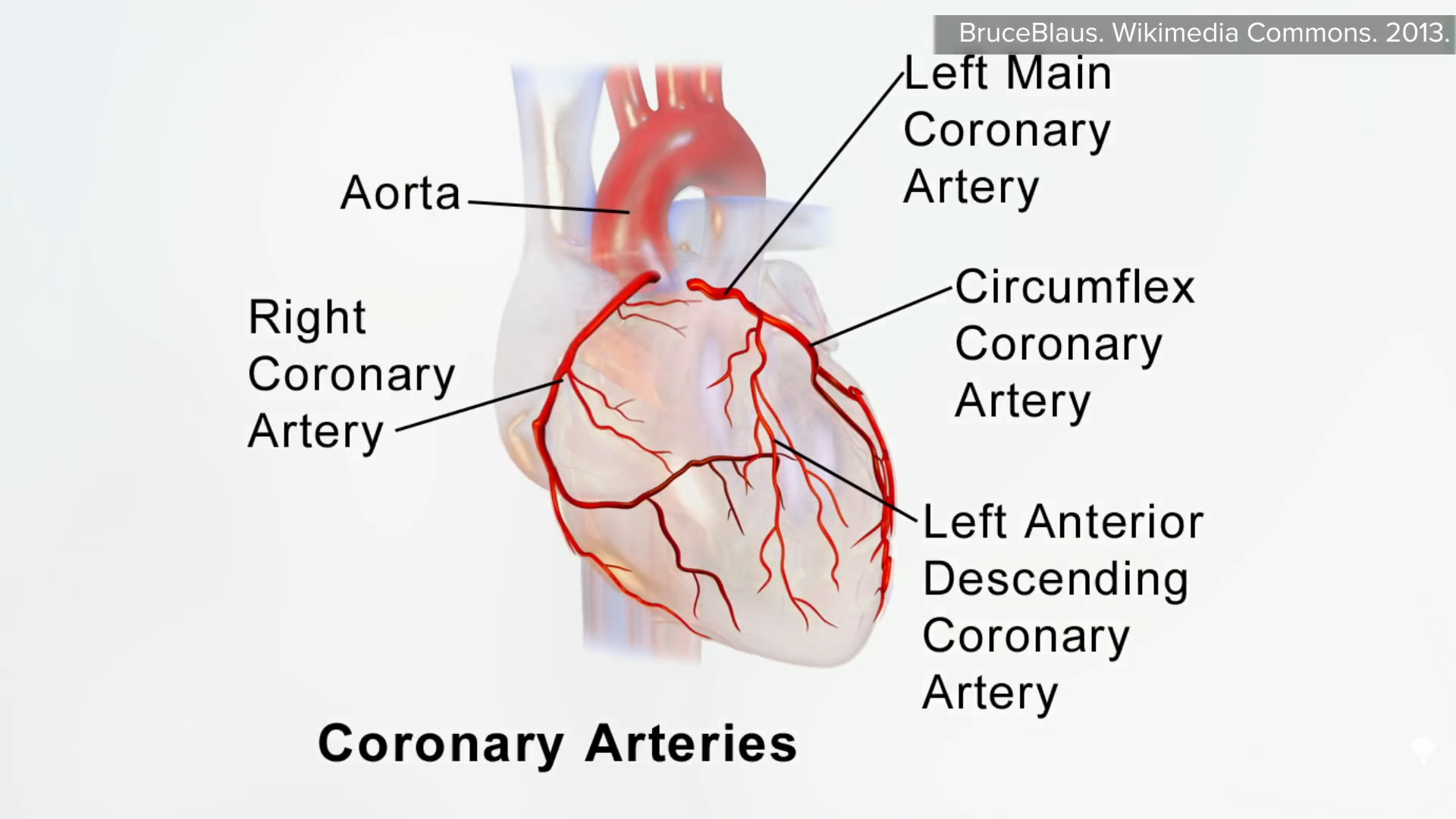
Four main coronary arteries feed the heart—the right coronary artery, the left main coronary artery, the circumflex coronary artery, and the left anterior descending coronary artery, as seen here and at 6:00 in my video.
If we add up their lengths, that’s about 11 inches (28 cm) of coronary arteries, which, for examination, can be cut into about 50 quarter-inch (5-mm) slices. Shown below and at 6:17 in my video is what is seen: Plaque isn’t gunking up one or two slivers but throughout all the coronary arteries. If we look at more than a thousand of these slices from dozens of patients who died of heart attacks, “not a single segment was devoid of plaque.” So, it’s no wonder that stenting open in just one area has no impact on heart attacks or death.